Reimagine growth at Elevate – Dallas 2025. See the Agenda.
Filter
Displaying 91-100 of 353




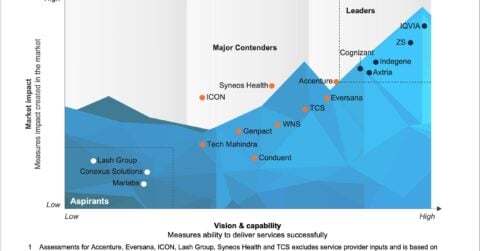
Revenue Cycle Management Trailblazers | Market Insights™
 by Ankur Verma
and 4 others
by Ankur Verma
and 4 others