Reimagine growth at Elevate – Dallas 2025. See the Agenda.
Who We Serve
We strengthen bold leaders – from the world’s largest companies to ambitious disruptors – helping them outpace the competition and shape the future.
What We Offer
Our memberships, custom support, and in-depth published research equip you with the reliable information you need to make data-led decisions with measurable success.
Our Expertise
We blend deep industry expertise with leading-edge research driving growth, innovation, and resilience. With Everest Group, data meets strategy, and vision turns into measurable impact.
Insights
Our wealth of resources inspires ideas and new ways of thinking with real-world solutions and the latest trends that drive your business forward.
Company
We’re committed to helping you get it right. Through trusted expertise, rigorous research, and practical insights, we enable businesses to make confident decisions.
Filter
Displaying 11-20 of 69
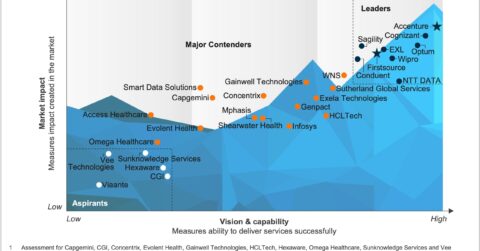
Healthcare Payer Digital Services PEAK Matrix® Assessment
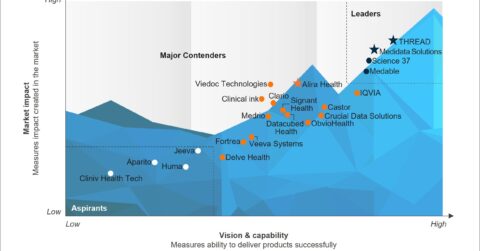
Decentralized Clinical Trial Platforms PEAK Matrix® Assessment
MedTech Operations PEAK Matrix® Assessment
Patient Engagement Platforms PEAK Matrix® Assessment
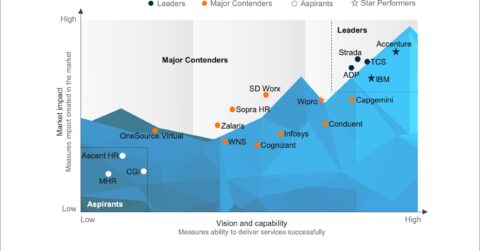
Multi-Process Human Resources Outsourcing (MPHRO) Services PEAK Matrix® Assessment
Clinical and Care Management Operations – Services PEAK Matrix® Assessment
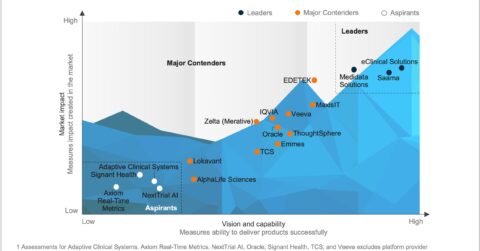
Life Sciences Clinical Data and Analytics (D&A) Platforms PEAK Matrix® Assessment
Healthcare Payer Operations PEAK Matrix® Assessment
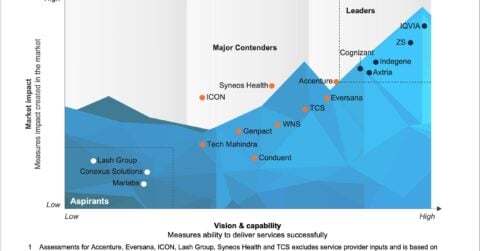
Life Sciences Sales and Marketing Operations – Services PEAK Matrix® Assessment
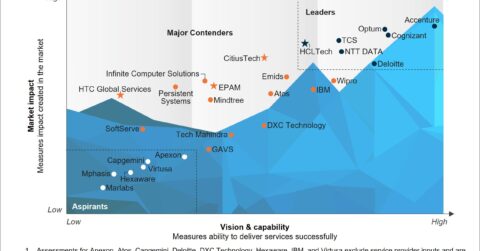
Healthcare Provider Digital Services PEAK Matrix® Assessment